
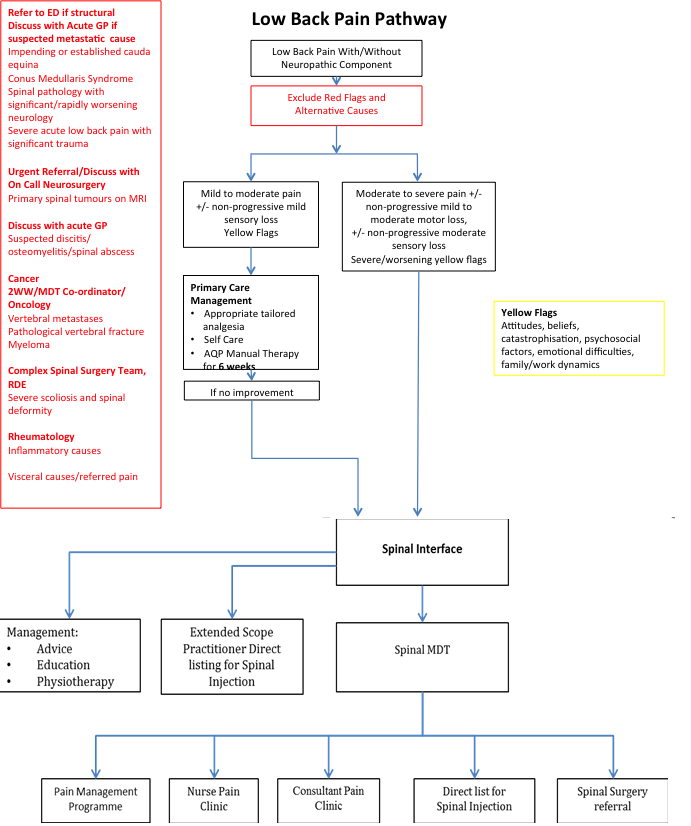
Adult Low Back Pain Guidelines
Red Flags/High Complexity Causes
Expediting Spinal Neurosurgery Referrals
Please note this guideline is for Lumbosacral Spine conditions only
Cervical and Thoracic cases are excluded and should be referred to Pain Clinic or Neurosurgery Depending On Clinical Requirement
Please note an MRI is required for all Neurosurgical referrals
Red Flags/High Complexity Causes:
The Cauda Equina Pathway Remains Unchanged
For Impending/Established Cauda Equina
Refer to Emergency Department
“A patient presenting with back pain and/or sciatic pain with any disturbance of their bladder or bowel function and/or saddle or genital sensory disturbance or bilateral leg pain should be suspected of having a threatened or actual Cauda Equina Syndrome”
British Association of Spine Surgeons (2018)
Cauda Equina Syndrome (CES) is a collection of patient symptoms and clinical signs. No single symptom or sign is pathognomonic. Some of the features may include:
Back Pain and / or Sciatic Pain with:
- New (within 2 weeks) difficulty initiating micturition or impaired sensation of urinary flow
- New (within 2 weeks) Altered Perianal, perineal or genital sensation S2-S5 dermatomes – area may be small or as big as a horse’s saddle (subjectively reported or objectively tested)
- Severe or progressive neurological deficit of both legs, such as major motor weakness with knee extension, ankle eversion, or foot dorsiflexion
- New (within 2 weeks) Loss of sensation of rectal fullness
- New (within 2 weeks) Sexual dysfunction (achievement of erection or ability to ejaculate, loss of vaginal sensation)
- Sudden Onset Bilateral Radicular Leg Pain (sciatica) or unilateral radicular leg pain that has progressed to bilateral
Conus Medullaris Syndrome
- Sudden and bilateral neurological deficit of the legs such as major motor weakness
- Symmetrical and bilateral perianal numbness
- Early onset urinary retention, overflow urinary incontinence and faecal incontinence
- Unexpected laxity of the anal sphincter
- Recent-onset erectile dysfunction frequently associated
Please note patients can present with a combination of these syndromes
The following presentations also require emergency referral to ED:
-
Spinal pathology with significant/rapidly worsening motor/sensory/sphincter disturbance
-
Severe acute low back pain straight after significant trauma – consider unstable vertebral fracture as cause
- Visceral causes: Ruptured AAA, Aortic dissection
Suspected metastatic spinal cord compression higher than cauda equina needs to be admitted under medicine via AcuteGP
Urgent Referral/Discuss With On Call Neurosurgery either by phone or via www.referapatient.org depending upon clinical urgency
-
Primary spinal tumours found on MRI imaging
-
Low back pain with sustained slowly progressive motor or sensory loss with cauda equina/conus medullaris and red flags excluded
-
Late complication directly related to recent Spinal Surgery even if discharged from follow up
- Please note an MRI is required for all Neurosurgical referral letters
Discuss with On Call Neurosurgery On Call by phone or via www.referapatient.org depending upon clinical urgency
-
Suspected Discitis
-
Suspected Osteomyelitis
- Suspected Spinal Abscess
If Vertebral Metastases/Pathological Vertebral Fracture
Suspected Primary Cancer Refer 2WW
Known Primary Cancer and Active Treatment MDT Cancer Co-ordinator
Unknown Primary Site Urgent Oncology
Common metastases to bone: Breast, Lung, Thyroid, Renal, Prostate, Melanoma
Myeloma 2WW/Urgent referral depends upon clinical severity
In The Absence Of Red Flags/High Complexity Diagnoses To Consider:
- Mechanical back pathology: Sciatica, Spinal stenosis, Disc prolapse/annular tears
- Non-pathological vertebral fractures
- Spondylolithesis
- Spondylosis
- Severe scoliosis and spinal deformity - Complex Spinal Surgery Team, Royal Devon & Exeter
-
Inflammatory causes
https://rms.cornwall.nhs.uk/primary_care_clinical_referral_criteria/primary_care_clinical_referral_criteria/rheumatology/inflammatory_back_pain_in_adults -
Visceral causes/Endocarditis/PE/Shingles/Post herpetic neuralgia/Aortic aneurysm/Metabolic bone disorders
This is NOT an Urgent Service, Routine referrals only.
Spinal Interface is a single point of access assessment service for all referrals.
Following assessment patients can be:
- Provided advice, education and physiotherapy
- Directly listed for spinal injection if meets specific criteria
-
Discussed in MDT for:
- Direct listing for spinal injection
- Consultant Pain Clinic Appointment
- Nurse Pain Clinic Appointment
- Referred for neurosurgery
Please note all low back pain referrals for further intervention require assessment at Spinal Interface first. Direct low back pain referrals for Spinal MDT, Spinal Injection/Intervention, Pain Clinic or Spinal Surgery will NOT be accepted.
Referral Criteria
- Mild to moderate spinal and/or radicular pain
- WITH/WITHOUT non-progressive mild sensory loss not responding to appropriate tailored medication, self care AND AQP manual therapy for at least 6 weeks
- Moderate to severe spinal and radicular pain
- WITH/WITHOUT non-progressive mild to moderate power loss
- WITH/WITHOUT moderate sensory loss
- Diagnosis uncertain, but serious pathology not suspected
- Severe/worsening yellow flags or persistent yellow flags not responding to initial primary care management/manual therapy
- Previous spinal surgery input and has been discharged from surgical follow up
Exclusions
- Cauda equina/conus medullaris syndrome
- Red flag pathology
- Rapidly deteriorating neurology
- Proven neoplasm
- Under 18 years
- Recent Spinal Surgery or Spinal Cord Stimulator under Pain Services in the same region and has not been discharged from Surgical or Pain Services follow up
- Cervical pathology or thoracic pathology – refer these to Pain Clinic or Spinal Surgery depending upon clinical need
- Widespread inflammatory disease
- Coccydynia
- Lumps/bumps
If an MRI has been performed prior to referral to Spinal Interface, please attach a copy of the report to the referral
Referrals For Consideration Of Spinal Injections
Please follow the Adult Low Back Pain pathway for all referrals. The Spinal Interface Service and MDT follow a unified policy on Spinal Injections and Radiofrequency Denervation developed and agreed by both Devon and Kernow CCGs. These can be accessed here
In summary:
Spinal Injection therapy can be commissioned if:
Patients with severe sciatica with or without low back pain with corresponding level of spinal pathology on clinical assessment and imaging, not improved with non-pharmacological and pharmacological treatments as per the Adult Low Back Pain pathway and part of a MDT plan
Exclusions:
Spinal injections for sciatica should not be repeated if performed less than 6 months earlier
Epidural injections for neurogenic claudication for patients with central canal stenosis
Patients with non-specific low back pain that is not associated with a corresponding level of spinal pathology or serious identifiable causes on clinical assessment and concordant imaging
Radiofrequency denervation is a specialist decision following assessment in Spinal Interface and MDT, please follow the Adult Low Back Pain guidelines. Repeated radiofrequency denervation will only be commissioned when the previous procedure was more than 16 months earlier and the origin of the pain is in the same location.
Expediting Spinal Neurosurgery Referrals
Please specify the reasons why the patient needs to be expedited in detail for example:
- Details of progression of motor and/or sensory deficits
- Details of change in distribution of pain
- Extent of worsening pain including level of distress caused and details of analgesia tried including neuropathic agent use
- Extent of functional impairment
If the patient is already under Spinal Interface Service
Please copy the corresponding team into the expedite letter.
Spinal Interface are happy to be contacted about any expedite queries for their patients not requiring immediate Spinal Surgical attention by email to:
spinal.interface@nhs.net (Three Spires)
cft.mskspinalinterface@nhs.net (CPFT)
Please note expedite requests that do not contain detailed reasons will be returned for further clarification.
Self Help
Tailored to individual needs/capabilities information and advice, address expectations, mobilise, return to work/social/leisure activities as possible
Back pain | The Chartered Society of Physiotherapy (csp.org.uk)
Analgesia
NICE Low Back Pain And Sciatica In Over 16s Recommendations Updated 2020
- Do not offer paracetamol alone for low back pain
- Consider NSAIDs taking into account individual risk factors for GI, renal and cardiac toxicity, concomitant medication and co-morbidities, consider gastro protection and ongoing monitoring of risk factors. Prescribe lowest dose for shortest time possible
- For acute low back pain consider weak opioids with or without paracetamol if an NSAID is contraindicated, not tolerated or ineffective
- Do not offer strong opioids, gabapentinoids, antiepileptics, SSRIs, SRNIs or TCAs for managing back pain
- Do not offer opioids for chronic sciatica or chronic low back pain
- For sciatica do not offer gabapentiniods, other antiepileptics, benzodiazepines or oral corticosteroids as there is no evidence of benefit and there is evidence of risk of harm
- If a person is already on opioids, gabapentinoids or benzodiazepines for sciatica, explain the risks of continuing them and participate in shared decision making about safe withdrawal of them using resources such as Opioids Aware | Faculty of Pain Medicine (fpm.ac.uk)
NICE Recommendations For Neuropathic Pain
The STarT back tool can help identify those at risk of chronic pain
Chronic Pain Management Resources For Patients And Clinicians
Detailed local resources for patients and clinicians on self-management, risks and benefits of drug prescribing and alternatives to medication
https://www.eclipsesolutions.org/Cornwall/info.aspx?bnfotherid=7
Occupational
Self refer to Occupational Health if restricting/unable to work. Promote and facilitate return to work and activities of daily living.
NB. Belts, corsets, foot orthotics, rocker sole shoes, peripheral electrical nerve stimulation and TENS machines are not recommended by NICE
Cognitive Functional Therapy
Evidence based service to help patients cope with stable, chronic lumbar back pain without radiation, red flags, pathology or neurological features. See here
In the absence of red flags/suspicion of vertebral fracture, plain X rays are not routinely indicated.2
MRI Guidelines - See Here
Patients with yellow flags often do well with early referral to physiotherapy (Attitudes, beliefs, catastrophisation, psycho-social factors, emotional difficulties, family/work dynamics)
Referral Criteria
Whiplash, stiffness and restricted movement, muscular neck and low back pain +/- non-progressive mild sensory loss, yellow flags, degenerative pain, postural neck and back pain, cervicogenic headaches
Exclusions
Suspected serious pathology, under 16, women over 35 weeks pregnant, patients not registered with a GP in locality
Patients who at initial assessment have little or no potential for further or sustained improvement through undertaking a course of treatment
Housebound patients
Patients with widespread or chronic (>1 year) musculoskeletal pain
Patients with a primary peripheral limb problem with secondary back and neck pain eg. Hip or shoulder problems, foot or gait abnormalities
Patients already seen by AQP in the preceding 12 month period (unless it can be justified that the initial package of care should be re-opened)
British Association of Spinal Surgeons (BASS) patient information leaflets on invasive interventions from facet joint injections to surgical procedures
http://www.spinesurgeons.ac.uk/patients-area/patient-information/
NHS Choices Lumbar Decompression Surgery patient information leaflet
http://www.nhs.uk/Conditions/Lumbardecompressivesurgery/Pages/Whatisitpage.aspx
Date Review : 19/10/2021
Next Review: 19/10/2022
GP Sifter: Dr Rebecca Hopkins
Version 1.5
Contributors
Dr. Natalie Dawes, GP and CCG Lead Orthopaedics
Janine Kennedy, Extended Scope Spinal Physiotherapist, Spinal Interface
Steve Iliffe, Extended Scope Spinal Physiotherapist, Spinal Interface
Dr. Robert Searle, Consultant Anaesthetist, Pain Clinic, Royal Cornwall Hospitals NHS Trust
Dr. Tom Sulkin, Consultant Radiologist, Royal Cornwall Hospitals NHS Trust
Mr. Andrew Clarke, Consultant Orthopaedic Spinal Surgeon, Royal Devon and Exeter
Dr. Rebecca Hopkins, GP and RMS Guidelines Lead Orthopaedics
References
- Integrated Spinal Pain and Non Spinal Triage Service, Neurosurgery, Derriford
- Low Back Pain and Sciatica In Over 16s Guideline. National Institute of Clinical Excellence. November 2016
- National Low Back and Radicular Pain Pathway 2017. NHS England 20 February 2017
- Opioids Aware, Faculty of Pain Management
- Drug Driving And Medicine: Advice For Healthcare Professionals. Department of Transport 2014
- SB Tool Online. STaRT Back Tool, Keele University, 2007
- MRI Guidelines
- Spinal Injections In Pain Clinic. Royal Cornwall Hospital Truro, December 2015
- What The Pain Clinic Offers. Kernow Referral Management Service Pain Clinic Guidance
- Patient Information Booklets. British Association Of Spinal Surgeons 2017
- Lumbar Decompression Surgery. NHS Choices, 2015
- NBP-CN: National Backpain Pathway – Clinical Network (2020) Early Recognition of Cauda Equina Syndrome: A Framework for Assessment and Referral for Primary care / MSK interface services